Vaccine Safety:
Current and Future
Challenges
Robert T. Chen MD, MA
Chief, Vaccine Safety and
Development Activity
Beth Hibbs RN, MPH
National Immunization Program (E-61)
Centers for Disease
Control and Prevention (CDC)
Atlanta, GA 30333
Educational Objectives
1. Discuss the importance of vaccine safety research. |
Introduction
Immunizations are responsible for preventing death and disability from disease and are among the most cost-effective and widely used public health interventions. However, it is also recognized that no vaccine is perfectly safe or effective. Some people will experience side effects from vaccines, and a few may not experience a complete immunologic response to a vaccine, leaving them susceptible to disease. Sustaining high vaccine coverage rates may become more of a challenge as people question the limitations of vaccines and new parents no longer see or hear about the diseases from which vaccines protect them. In the future, maintaining public support for immunizations will be critical for preventing outbreaks of vaccine preventable diseases. In this chapter, we will focus on the importance of vaccine safety research; current gaps and limitations in knowledge in the field of vaccine safety; how vaccine safety is monitored; the vaccine injury compensation program; vaccine risk communication, and helpful resources for specific questions about vaccine safety.
The Importance of Ongoing Vaccine Safety Research
Vaccine adverse event reports include health events caused by vaccines (i.e., true adverse reactions) and those that are not caused by vaccines (associated only by coincidence). In maturing immunization programs, (figure 1) close monitoring and timely assessment of suspected vaccine adverse events are critical to prevent loss of confidence, decreased vaccine coverage, and return of epidemic disease. 1,2 This has been experienced in several countries for pertussis,3 and more recently, diphtheria. 4
Figure 1. Evolution of immunization program and prominence of vaccine safety.There are several key considerations for supporting and maintaining an active vaccine safety program. First, a higher standard of safety is generally expected of vaccines than of other medical interventions because, in contrast to most pharmaceutical products, which are administered to ill people for curative purposes, vaccines are generally given to healthy people to prevent disease. Public tolerance of adverse reactions related to products given to healthy people, especially healthy babies, is substantially lower than to products administered to people who are already sick.5 This lower risk tolerance by the public for vaccines translates into a need to investigate rarer possible causes of adverse events following vaccinations than would be acceptable for most other pharmaceutical products.
Another consideration is based on the widespread use of vaccines and the potential extensive impact of problems or concerns to develop in a large percentage of the population that receives them.6 An example of this potential impact can been seen in recent concerns that polio vaccine contaminated by simian virus 40 may have been received by millions of people during the 1950's.7 Another concern recently expressed in Britain was the possibility that vaccines may have contained gelatin stabilizers produced in cattle infected with bovine spongiform encephalopathy. 8 The importance of ensuring the safety of a relatively universal human-directed "exposure" like immunizations is the basis for strict regulatory control of vaccines by the Food and Drug Administration (FDA) in this country.9 A high standard for vaccine safety is also needed, because providing a record of immunization is mandated under many state and local school entry requirements.
Unlike many classes of drugs for which other effective therapy may be substituted, vaccines generally have few alternative strains or types to chose from. The decision to withdraw a vaccine or switch between strains may also have wide ramifications. For example, the withdrawal of the 1976 "swine influenza" vaccine due to elevated risk of Guillain-Barré syndrome led to many lawsuits and low public acceptance for influenza vaccinations for a decade.10 Establishing associations with vaccines and promptly defining the attributable risks are critical in placing adverse events in the proper risk-benefit perspective. An erroneous association or attributable risk can undermine confidence in a vaccine and have disastrous consequences for vaccine acceptance and disease incidence. On the other hand, denials of association despite accumulating evidence can also undermine public confidence. 11,12 Research in vaccine safety can help to distinguish true vaccine reactions from coincidental unrelated events and may help to maintain public confidence in immunizations and the credibility of immunization programs.
Limitations and Gaps in the Science of Vaccine Safety
In 1967, the lack of scientific documentation on the hazards of immunization moved Sir Graham Wilson, former director of the Public Health Laboratory Service in the U.K., to compile the first vaccine safety review. He noted fear of compensation claims or inadvertent support to "anti-vaccinationaists" as possible explanations for the incomplete records.5
In the United States, The National Childhood Vaccine Injury Act of 1986 established a Committee from the Institute of Medicine (IOM) to review the adverse consequences of childhood vaccines. This group found severe limits in the knowledge and research capability on vaccine safety. Of the 76 vaccine adverse events they reviewed for causal relation, 50 (66%) had no or inadequate research. Specifically, the IOM Committees identified the following limitation's: 1) Inadequate understanding of biologic mechanisms underlying adverse events; 2) Insufficient or inconsistent information from case reports and case series; 3) Inadequate size or length of follow-up of many population-based epidemiologic studies; 4) Limitations of existing surveillance systems to provide persuasive evidence of causation and 5) Few experimental studies published relative to the total number of epidemiologic studies published.13,14
Vaccine safety research requires expertise in "rare disease" epidemiology.15,16 Such studies are costly and difficult to organize and may be less familiar to most immunization experts with mainly an infectious disease background. Like other areas of safety (e.g., food), vaccine safety cannot be studied directly. Typically, vaccine safety studies that are epidemiologically based are inferred by the sum of the inverse: an absence of specific problems when appropriate surveillance and risk management systems are in place. Scientifically, it is more challenging to prove than disprove a concept, especially a negative concept.17
The IOM concluded that "if research capacity and accomplishments [are] not
improved, future reviews of vaccine safety [will be] similarly handicapped."
Although much remains to be done, much progress has been made the past few years
toward understanding these gaps and ameliorating the research infrastructure to
improve vaccine safety. 1,2,18-22
Methods of
Monitoring Vaccine Safety
The importance of ensuring vaccine safety encompasses a broad range of activities. Pre-licensure evaluations and post-licensure surveillance systems are in place at the federal level. Safety issues regarding the storage, handling, and recording of vaccines by individual clinicians are also an important component in considerations in vaccine safety.
Pre-licensure
Like other pharmaceutical products, vaccines, undergo extensive safety and efficacy evaluations in the laboratory, in animals and in sequentially phased human clinical trials prior to licensure.9 Phase I trials usually number in the tens and can only detect the grossest toxicity. Phase II trials generally enroll hundreds of people and, when carefully coordinated, can provide important conclusions. These conclusions might address the relationship between the concentration of antigens, number of vaccine components, formulation technique, effect of successive dose and profile of common reactions, all of which impact on the choice of the vaccines chosen for Phase III trial.23,24 The sample size for Phase III vaccine trials are based primarily on efficacy considerations, usually ranging between 100 and 10,000 participants. The maximum duration of observation is also generally limited to a couple of years. The availability of unvaccinated control group, however, allows clear identification of true common local and systemic reactions (e.g., injection site swelling, fever, fussiness).23 To identify potential safety problems, vaccines go through pre-release lot testing for safety and potency.9,25 This evaluation usually occurs parallel to the clinical trials prior to vaccine licensure.
Post-licensure
Vaccines are also monitored for safety in multiple ways after they are released for public use. Because rare reactions, delayed reactions, or reactions within sub-populations may not be detected before vaccines are licensed, post-licensure (also called post-marketing) evaluation of vaccine safety when millions of persons may be vaccinated is critical. Historically, this has relied on passive surveillance systems like the Vaccine Adverse Event Reporting System (VAERS) and ad hoc epidemiologic studies. More recently, Phase IV trials and pre-established large-linked databases (LLDBs) have been added to improve our methodology capabilities to study rare risks of specific immunizations.15 Furthermore, because vaccines are biologic rather than chemical in nature, variation in rates of adverse events (and immunogenicity) by manufacturer, 26,27 or even by lot might be expected.28 Post-licensure surveillance systems may detect potential lot-specific irregularities in a timely manner.
Passive Surveillance (Spontaneous Reporting System)
Passive surveillance or spontaneous reporting system (SRSs) have been the cornerstone of most vaccine safety monitoring systems because of their relative low cost of operations.29,30 National reporting of vaccine adverse events can be done through the same reporting channels as those used for other adverse drug reactions.30 Vaccine manufacturers also maintain SRSs for their products, which are usually forwarded subsequently to appropriate national authorities.29
Due to the importance of infectious disease control, vaccines are purchased and administered by national public health authorities. For example, the public sector ( federal, state, and local governments) coordinates its programs with the Centers for Disease Control and Prevention (CDC). The CDC purchases and distributes more than half of the childhood vaccines administered in the United States. The CDC collaborated with FDA, which licenses and regulates vaccines, in developing the Vaccine Adverse Event Reporting System (VAERS).
The Vaccine Adverse Event Reporting System (VAERS)
VAERS is known as a passive surveillance system because it depends on health care providers and/or patients and others to file adverse event reports. The National Childhood Vaccine Injury Act of 1986 mandated, for the first time, that health providers report certain adverse events after immunizations.31 VAERS was implemented jointly by the CDC and FDA in 1990 to provide a unified national system for collection of all reports of clinically significant adverse events, including but not limited to those mandated for reporting.1 The creation of VAERS also provided an opportunity to correct some shortcomings of the predecessor CDC Monitoring System for Adverse Events Following Immunizations (MSAEFI) and FDA Adverse Drug Reaction. 32
 Figure 2. Reported vaccine-preventable diseases (VPD) and reports to VAERS,
1991-1997.
Figure 2. Reported vaccine-preventable diseases (VPD) and reports to VAERS,
1991-1997.The VAERS reporting form is designed to allow a narrative description of adverse events. All persons, including patients, parents (constitute less than 5% of VAERS reports), and health professionals, can report to VAERS. There are no restrictions on onset intervals or requirements for medical care. Annually, VAERS forms are sent to approximately 200,000 physicians in the specialties of pediatrics, family practice, general practice, internal medicine, obstetrics/gynecology, and emergency medicine. Copies are also sent to state health departments and to public clinics that administer vaccines. Information sought on the VAERS report include the vaccine received, the timing of the vaccination and the onset of adverse events, demographic information about the recipient, information about concurrent medical illnesses or medications, and past history of adverse events after vaccination. The form is preaddressed and postage-paid so that after completion it can be folded and mailed. To request a VAERS form, assistance in completing the form, or answers to other questions about the reporting system, call 1-800- 822-7967.
A contractor, under CDC and FDA supervision, distributes, collects, codes (using the Coding Symbols for a Thesaurus of Adverse Reaction Terms) (COSTART), and enters VAERS reports in a database. A verification-of-receipt letter, bearing the assigned VAERS identification number is returned to the reporter. Reporters of selected serious events receive written requests from VAERS (60 days after vaccination and one year after vaccination) for information about the patient's recovery. Reporters may also submit additional relevant information to the VAERS by using the assigned identification number. Both the CDC and FDA have online computer access to the VAERS database and focus their efforts on analytical tasks of interest to their respective agencies. These data (minus personal identifiers) are also available to the public.
Classifications, Case Definitions and Evaluative Protocols
Vaccine reactions can be classified by frequency (common, rare), extent (local, systemic), severity (hospitalization, disability, death), causality, and preventability (intrinsic to vaccine, faulty production, faulty administration). A recent classification divides adverse events after vaccinations:34,35
1. Vaccine-induced: due to the intrinsic characteristic of the vaccine preparation and the individual response of the vaccinee, these events would not have occurred without vaccination (e.g., vaccine-associated paralytic poliomyelitis).
2. Vaccine-potentiated: the event would have occurred anyway, but was precipitated by the vaccination (e.g., first febrile seizure in a predisposed child).
3.Programmatic error: the event occurred due to technical errors in vaccine preparation, handling, or administration.
4. Coincidental: the event was associated temporally with vaccination (e.g. by chance occurrence or due to underlying illness).
To further improve the quality of SRS data and maximize its utility as a registry of rare potential vaccine reactions, standard protocols for the clinical evaluation of selected serious events reported to VAERS (e.g., deaths, seizures) are under development. Such protocols could then be sent to the health care providers who report such events in order to standardize the evaluation of these patients.
Assessment of Causality of Vaccine Adverse Events
The formal process of assessing causality of an adverse event and an exposure (e.g., vaccine) is a complex process that can be considered in terms of the answers to three questions: Can It?, Did It?, and Will It?13,14,36 For individual case reports, the "Did It?" question is more relevant. If the answer is yes, then "Can It?" is also answered in the affirmative. It is natural to suspect the vaccine to be the cause when an adverse event occurs following vaccination, but in reality a causal association may or may not exist. Information used for assessing causality in individual case reports includes the following: a) previous general experience with vaccine; b) alternative etiologies; c) susceptibility of the vaccinee; d) timing of events; e) characteristic of the event (e.g., confirmatory laboratory findings); f) dechallenge; g) rechallenge.
When a vaccine can cause an adverse event, the question "Will It?" refers to the probability that an individual will experience the event or, for populations, the proportion that will experience it (i.e., the attributable risk). These data are critical for risk-benefit considerations and are generally available only when the "Can It?" question is answered based on epidemiologic studies? 14
Another approach to causality that minimizes controversy is to assume that adverse events that occur within a particular period after vaccinations are caused by the vaccine, irrespective of whether they were truly causal or just coincidental. This approach to causality is used in some vaccine injury compensation programs to simplify the proceedings.37 Classifications are based on the reported symptoms, the interval between vaccination and onset of symptoms, and a set of case definitions.
Usually, causal link between the vaccine and an adverse event can be established if there is a unique laboratory diagnostic result (e.g., viral culture in patient with adverse event and genetic sequencing showing virus is a vaccine and not a wild strain);38 a unique clinical syndrome (e.g., acute flaccid paralysis classical for polio occurring shortly after receipt of oral polio vaccine in setting where wild polio virus circulation is unlikely);39 or an epidemiologic study showing vaccinated people are more likely than unvaccinated people to experience the adverse event. Unfortunately, very few VAERS reports meet either of the first two criteria.
 Figure 3. Establishing a causal link: adverse event and vaccine.
Figure 3. Establishing a causal link: adverse event and vaccine.Large-Linked Databases (LLDB)
Historically, when a signal of a potential vaccine safety concern was generated from passive surveillance, ad hoc epidemiologic studies were needed to test this hypothesis. Such ad hoc studies while, potentially informative about vaccine causality, are costly, time-consuming, and usually limited to assessment of a single hypothesis.
The limitations of VAERS and the recognition of the need for improved monitoring of vaccine safety prompted the CDC to initiate the VSD project in 1990.22 To help overcome the previously identified shortcomings, the VSD study prospective collects vaccination, medical outcome (e.g., hospital discharge, outpatient, emergency room, deaths), and covariant data (e.g., birth certificates, census) under joint protocol at multiple HMOs. Selection of staff model prepaid health plans also minimized potential biases resulting from data generated from fee-for-service claims. The VSD has conducted active surveillance on approximately 500,000 children from birth through 6 years of age (75,000 birth cohort, approximately 2% of U.S. population in these age groups) whose parents (or legal guardians) were enrolled in one of four staff model HMOs.22 Expansion to include all age groups in the study is underway. Each site encodes their patients' clinical data with unique study identifiers before sending to data to CDC annually for merging and analysis, thereby preserving patient confidentiality. Depending on the background incidence of the medical event, the frequency of specific vaccinations and their relative risk, associations of 1 per 100,000 doses should be detectable within 5 years.
The VSD has focused its initial efforts on examining potential associations between immunizations and 34 serious neurologic, allergic, hematologic, infectious, inflammatory, and metabolic conditions. The VSD is also being used to test new ad hoc vaccine safety hypotheses. These may arise from the medical literature,40 from VAERS,27 from changes in immunization schedules,41 or from the introduction of new vaccines.42 The diversity in vaccination practice at the four HMOs and the clinic-to-clinic and day-to-day variations in practice permit useful contrasts in safety experiences.41 The size of the VSD population may also permit separation of the risks associated with individual vaccines from those associated with vaccine combinations, whether given in the same syringe or simultaneously at different body sites. Such studies will be especially valuable in view of the new combined pediatric vaccines currently in development.43
Should the VSD study identify a vaccine reaction, data on attributable risk will be available, thereby permitting accurate risk-benefit assessment by both the public and policymakers.44 Subgroup analyses may permit identification of risk factors, which may be useful in identifying contraindications to vaccinations. The incidence rates of reactions identified in VSD should permit the evaluation and improvement of passive surveillance systems like VAERS. The VSD data can also aid the FDA27 and the Vaccine Injury Compensation Program.45
Amid these promises, a few caveats are appropriate. While diverse, the population in the four HMOs currently in the VSD is not wholly representative of the United States in terms of geography or socioeconomic status. More importantly, due to the high coverage attained in the HMOs for most vaccines, few nonvaccinated controls are available. The VSD must, therefore, rely predominantly on some type of "risk-interval" analysis.46,47 The capability of this approach to assess associations between vaccination and adverse events with delayed or insidious onset (e.g. autism) is limited. Similarly, the ability of the VSD to fully distinguish effects of combined or simultaneous vaccination may be limited should such practices become universal. The VSD also cannot easily assess adverse events not currently captured in existing HMO databases, either because they do not result in a health care consultation or because the data are not automated.22 The patient enrollment, health care practices, and health information systems at each HMO are dynamic, which may either aid or impede study of specific outcomes. Coding error occurs inevitably in all data files to some extent, resulting in a decrease in our ability to detect a true association. The current VSD is also unable to examine the risk of extremely rare events after infrequent vaccinations, such as Guillain-Barré syndrome, after each season's flu vaccine. Because the VSD relies on epidemiologic methods, it may not successfully control for confounding and bias in each analysis48 and inferences on causality may be limited.
Despite these potential shortcomings, the VSD provides a new, essential,
powerful, and cost-effective complement to our ongoing evaluations of vaccine
safety in the United States. In view of the methodologic and logistical
advantages offered by LLDBs, the United Kingdom and Canada have also developed
LLDBs, linking immunization registries with medical files.18,21
Because of the relatively limited number of vaccines used worldwide and the
costs associated with establishing and operating them, it is unlikely that all
countries will be able to or need to establish their own LLDBs. They should be
able to draw upon the scientific base established by the existing LLDBs for
vaccine safety and, if needed, to conduct ad hoc epidemiologic studies.
Vaccine Administration Considerations
In order to maintain their proper biologic activity, vaccines must be properly shipped, stored, and administered. Failure to adhere to these requirements can lead to loss of vaccine potency, resulting in an inadequate immune response to the vaccine.49 Proper storage and handling requirements for each vaccine are given on the manufacturer's information insert. This information can also be found in recommendations of the Advisory Committee on Immunization Practices of the CDC and the American Academy of Pediatrics. 50-52 Another concern is the growing complexity of vaccines (table 1), including the growing variety of multiple combination vaccines that clinics will be faced with keeping in clinic stock.53 These decisions will become more challenging, especially when patients change health care providers and the providers stock different vaccine combinations. To prevent administration errors, adequate and accurate recording of combination vaccines in patient charts will become increasingly important to ensure proper practices are followed. Immunization staff will continue to need education in appropriate vaccine storage, handling, and safe injection practices. 54
In developing countries, vaccine safety concerns frequently relate more to inadequate control of vaccine production and administration errors such as reuse of needles resulting in the transmission of blood-borne pathogens. It is anticipated, however, that as nations in both developed and developing countries reach high vaccine coverage and vaccine-preventable diseases become less visible, public concerns about vaccine safety may also threaten the stability of current immunization programs.3
Vaccine Injury Compensation Program
Because many vaccinations are mandated for public health reasons and because no vaccine is perfectly safe, several countries have established compensation programs for people who may have been injured by vaccination.37 During the 1980's in the United States, increases in reports about adverse events following vaccination led to an increased number of lawsuits against vaccine manufacturers.55 As a result, substantial increases in the price of vaccines began to occur as well as a loss of manufacturers willing to produce vaccines.56 Due to these disturbing trends, the National Childhood Vaccine Injury act of 1986 established the National Vaccine Injury Compensation Program. This program was designed to compensate those individuals or families of individuals who have been injured by childhood vaccines on a "no-fault" basis, based on a predetermined Vaccine Injury Table. Accurate assessments of whether adverse events can be caused by specific vaccines are required to update the Vaccine Injury Table as to justly compensate people injured by true reactions and to disallow false or unrelated claims.45 The program is administered jointly by the Department of Health and Human Services and the Department of Justice. To obtain an information packet on how to file a claim, criteria for eligibility, and documentation required, call 1-800-338-2382 or write to the National Vaccine Injury Compensation Program, Parklawn Building, Room 8A-35, 5600 Fishers Lane, Rockville, Maryland 20857.
Vaccine Risk Communication Considerations
Almost every child in this country is vaccinated, and therefore almost every parent has a question about vaccines. Parents want to know what vaccines are made of, if they work, and whether they are safe.57 Inaccurate or misleading information relating to vaccines is readily available to parents and can be found on the Internet and in some publications. The art of handling vaccine safety concerns and vaccine risk communication has emerged as an increasingly important skill for health care providers. Periodically, vaccine safety concerns also emerge in the media. The media aims to present both sides of a story and not judge the strength of one side over another. The challenge for healthcare professionals is to establish greater credibility with the audience in instances of inaccurate or misleading news reports.58,59
Health Risk communication has traditionally consisted of messages designed to encourage behavior that reduces individual and societal risk (e.g., smoking cessation).59 Risk communication is seen as an interactive process of an exchange of information and opinion among individuals, groups, and institutions.62 Risk communication, while having a 20 year history as a field of study, is still an emerging field in vaccine education. A big challenge in vaccine risk communication is acknowledging and defining uncertainty about the very small estimates of risk associated with vaccination. Risk communication is more effective when this uncertainty is stated and when risks are quantified as much as science permits. Trust is a key component of the exchange of information at every level, and overconfidence about risk estimates that are later shown to be incorrect contribute to a breakdown of trust among people involved.59,61 Disease prevention is a difficult task, especially when it requires participation by a majority of the population. In the pre-immunization era, vaccine-preventable diseases like measles and pertussis were so widespread that the risks and benefits of disease compared with vaccination were readily evident. As immunization programs successfully reduced the incidence of disease, an increasing number of health care providers and parents have had little or no personal experience with these once common diseases. These individuals are forced to rely on history and other more "distant" descriptions of these diseases in textbooks or educational brochures. In contrast, what is visible is the degree of very personal discomfort associated with each immunization.
Principles of Risk Communication
 Some key principles and lessons can be applied to vaccine risk communication:
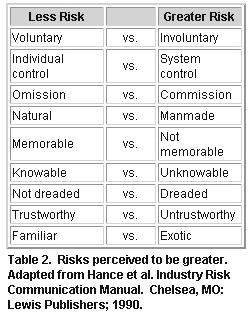
1) Individuals differ in their perceptions of risk depending on their life
experience and knowledge; 2) Certain risks are more acceptable to people than
other risks (table 2); and 3) Risk communication is an interactive process that
requires active listening and discussion.
Some key principles and lessons can be applied to vaccine risk communication:
1) Individuals differ in their perceptions of risk depending on their life
experience and knowledge; 2) Certain risks are more acceptable to people than
other risks (table 2); and 3) Risk communication is an interactive process that
requires active listening and discussion.
People who have had an adverse reaction or event following vaccination or know someone who has had a bad experience may perceive vaccinations as being more risky than those who have not. On the other hand, patients who have had a vaccine-preventable disease, like polio, and physicians who worked in polio wards in the 1950s are more likely to be stronger advocates of polio vaccination than patients or physicians who never saw wild polio disease. Personal stories can be a powerful influence and motivator, especially if they are emotional compelling.
In an analysis of Internet web pages of parent groups with concerns about vaccination, personal stories about adverse reactions believed to be associated with vaccines were one of the most frequently highlighted features. 62
Knowledge can also be a powerful influence in risk decisions. People may perceive a greater risk for things that they do not know about versus those things with which they are familiar. For instance, Measles vaccine may be perceived as less risky than a vaccine that sounds unfamiliar and exotic, such as Hib.
Identifying the source of a parent's information (e.g. news stories, alternative health, vaccine information statements, and office staff,) can help focus your interaction and is an important first step in the risk communication process. In informal discussions with parents who had concerns about vaccines at a recent parent conference focusing on vaccine safety, sources of parent information included a wide range of materials, including nontraditional health resources, which they perceived as being as credible as information from traditional sources. The perception of having knowledge to control the outcome of whether one's children become infected with vaccine-preventable diseases also affects the acceptance of vaccine risks. In one study, nonvaccinators believed they could prevent their children from catching whooping cough, and they also thought it was less likely that their child would be disabled or killed by disease in the absence of vaccination.63 Understanding a patient's source of information provides a key to an effective approach in correcting misconceptions about vaccines. In some cases, source correction, in addition to patient counseling, should be considered (for instance, writing a letter to the editor of a recent inaccurate news publication).
Another consideration in assessing knowledge is to recognize a person's learning style. One style used by people is to seek out a trusted source for information on vaccines; and for many people, this is their pediatrician. Another style is to seek out many different sources of information. Persons using this style will actively look for several different resources to confirm or expand their perceptions about a topic. In an analysis of calls coming into the National Immunization Hotline, several callers were confirming vaccine information that their physician had provided them with hotline staff. For some people, these confirmation behaviors become more pronounced in risk/benefit decisions. The more risky the perception, the greater the need to seek multiple opinions about the perceived risky behavior. Providing these people with several different resources they can go to in their learning process may be a helpful intervention (see the vaccine safety resource appendix for helpful references and resources that can be shared with patients).
Risk perceptions are individual; however, some risk are naturally more acceptable to people than others.64 The risk perception comparisons seen in figure 9 have been adapted from risk perceptions as they relate to environmental concerns, but can be applied to immunization practices as well. A discussion on a few of these and how they relate follows.
Voluntary risks are usually more acceptable than involuntary risks. For most people, assuming the risk of a vaccine side effect after a free, voluntary, company-offered, flu vaccine program is more acceptable than assuming the risk of a side effect from a company-required flu immunization program. Many state laws require vaccination upon school entry (system control), which can be perceived as more risky. Most of these states also offer religious and philosophical exemptions to vaccination, allowing for less risk (individual control).
For two equal risks, one due to an action and one due to inaction, most people prefer the consequences of inaction.63 That is to say, if there were an equal risk of a bad outcome from an action (such as an adverse reaction to vaccination) and inaction (such as getting a disease due to nonvaccination), many people have an "omission bias": they would prefer the consequences of omission to commission.
In the United States, information developed by the CDC about the risks and benefits of immunizations is required to be provided to all public sector people receiving vaccinations since 1978.65 Recent efforts have been devoted to the use of focus groups and other research to assess and improve the effectiveness of such information material. Studies on the use of positive versus negative framing to help people put risks in perspective have had good results.66,67 An example of positive framing is presenting the percentage of people who have no adverse reactions to vaccines instead of framing the statement negatively as the percentage of those who do. In many countries, including the United States, people who believe that their children or themselves have been injured by vaccines have organized to distribute through the Internet and various publications information that highlights the risks of and uncertainties related to immunizations. Materials to address these misconceptions and allegations about immunizations are developed by the National Immunization Program and distributed to state immunization programs as they arise. These materials can be obtained from the National Immunization Hotline (800) 232-2522 and the National Immunization Program Web Page (www.cdc.gov/nip). In the future, we will need to create better systems to assess concerns, develop and disseminate materials to address public needs, and develop present day and historically based materials that can express the impact of outbreaks of vaccine-preventable diseases.
Risk communication can be used for the purposes of either advocacy, public education, or decision-making partnership. People care not only about the magnitude of the risk, but also how the risks are managed and whether they participate in the risk-management process, especially in a democratic society.59,68 Immunization is unlike most other medical procedures, in that the consequences of the decision affect not only the individual but also others in the society. Because of this important distinction, many countries have enacted public health (e.g., immunization) laws that severely limit any individual's right to infect others. Some people may attempt to avoid the risks of vaccination while being protected by the group also known as herd immunity, which results from others being vaccinated. The protection provided by herd immunity may disappear if too many people avoid vaccination, which may result in tragic outbreaks of diseases. 3,69 Recent debates in the United States have focused on whether philosophical (in addition to medical and religious) exemptions to mandatory immunizations should be allowed more universally and, if so, what standards for claim of exemption are needed. Vaccine risk communication should discuss the risks and benefits of specific vaccines and should also inform people receiving vaccinations about the delicate balance between societal and individual rights in a shared community.
Evaluating and Managing Vaccine Safety Concerns
Empathy, patience, and a careful assessment are all needed to effectively address vaccine safety concerns from a clinical perspective. As with all investigations, the first step is objective and comprehensive data gathering with an open mind. Premature dismissal of a new vaccine safety concern as "unfounded" without gathering and weighing the evidence is unwise and unscientific. On the other hand, endorsement of isolated findings or unproven theories about vaccines without careful consideration to the weight of evidence can be equally problematic.
Establishing trust and credibility are key in promoting a positive relationship. Factors that aid in such credibility include careful assessment of the patient's concern, scientific and medical expertise, empathy, and the ability to distill scientific facts and figures down to easily understood concepts. Emotionally compelling first-hand accounts of the effects of vaccine-preventable diseases may be needed to effectively illustrate the importance of vaccination practices.
Clarifying the distinction between theory, fact and perceived and real risk
for the concerned public is critical. What is certain is the risk associated
with the vaccine-preventable disease should a person remain non-immune. What is
also certain is the small magnitude of risk for any severe vaccine reactions.
The significance of uncertainty in vaccine safety is related to individual
perceptions. Learning how to effectively communicate with patients will become
an increasingly important skill for health care providers in ensuring the
protection of our children from vaccine- preventable diseases.
References
1. Chen RT, Rastogi SC, Mullen JR, et al. The Vaccine Adverse Event Reporting System (VAERS). Vaccine. 1994;12:542-550
2. Duclos P.Surveillance des effets secondaires de la vaccination. Sante 1994;4:215-20.
3. Gangarosa EJ, Galazka AM, Wolfe CR, Chen RT, Phillips LM, Gangarosa, RE, Miller E. Impact of the anti-whole-cell pertussis vaccine movements. Lancet 1997;351:356-361.
4.Galazka AM, Robertson SE, Oblapenko GP. Resurgence of diphtheria. Eur J Epidemiol. 1995;11:95-105.
5. Wilson GS. The hazards of immunization. London: Athlone Press, 1967.
6. Schumacher W: Legal/ethical aspects of vaccinations. Develop biol Standard 1979; 43:435-8.
7. Pennisi E. Monkey virus DNA found in rare human cancers. Science 1997;275:748-9.
8. Food and Drug Administration. Bovine-derived materials: Agency letters to manufacturers of FDA-regulated products. Federal Register 1994;59:44591-4.
9. Mathieu M, ed. Biologic development: a regulatory overview. Waltham MA: Paraxel, 1993.
10. Neustadt RE, Fineberg HV: The swine flu affair: decision-making on a slippery disease. Washington DC: US Government Printing Office, 1978.
11. Lloyd JC, Chen, RT. The Urabe mumps vaccine: lessons in adverse event surveillance and response. Pharmacoepidemiology and Drug Safety. 1996; 5:S45. Abstract.
12. Kimura M, Kuno-Sakai H, Yamazaki S et al. Adverse events associated with MMR vaccines in Japan. Acta Paediatrica Japonica 1996;38:205-11.
13. Howson CP, Howe CJ, Fineberg HV, eds. Institute of Medicine. Adverse effects of pertussis and rubella vaccines: A report of the Committee to Review the Adverse Consequences of Pertussis and Rubella Vaccines. Washington, D.C.: National Academy Press; 1991.
14. Stratton KR, Howe CJ, Johnston RB, eds. Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality. Washington D.C.:National Academy Press; 1994.
15. Chen RT. Special methodological issues in pharmacoepidemiology studies of vaccine safety. In: Strom BL, ed. Pharmacoepidemiology. Sussex: John Wiley & Sons, 1994:581-94.
16. Fine PEM, Chen RT. Confounding in studies of adverse reactions to vaccines. Am J Epidemiol. 1992;136:121-135.
17. Rothman KJ, ed. Causal inference. Chestnut Hill, MA: Epidemiology Resources, Inc; 1988.
18. Farrington CP, Pugh S, Colville A, et al. A new method for active surveillance of adverse events from diphtheria/tetanus/pertussis and measles/mumps/rubella vaccines. Lancet. 1995;345:567-569.
19. Ellenberg SS, Chen RT. The complicated task of monitoring vaccine safety. Public Health Reports 1997;112:10-20.
20. Morris R, Halperin S, Dery P et al. IMPACT monitoring network: a better mousetrap. Can J Infect Dis 1993;4:194-5.
21. Roberts JD, Roos LL, Poffenroth LA, et al. Surveillance of vaccine-related adverse events in the first year of life: A Manitoba cohort study. J Clin Epidemiol. 1996;49:51-58.
22. Chen RT, Glasser J, Rhodes P, et al. The Vaccine Safety Datalink Project:
A New Tool for Improving Vaccine Safety Monitoring in the United States.
Pediatrics 1997;99:765-73.
23. Rosenthal KL, McVittie LD. The clinical
testing of preventive vaccines. In: Mathieu M, ed. Biologic development: a
regulatory overview. Waltham MA: Paraxel, 1993:119-30.
24. Pinichiero ME. Acellular pertussis vaccines: towards an improved safety profile. Drug experience 1996;15:311-24.
25. Global Programme on Vaccines and Immunization. Quality: the first consideration. Geneva: WHO/GPV/SAGE.97/WP.03.
26. Steinhoff MC, Reed GF, Decker MD, et al. A randomized comparison of reactogenicity and immunogenicity of two whole-cell pertussis vaccines.Pediatrics 1995 S567-70.
27. Niu MT, Rhodes P, Salive M, Lively T, Davis DM, Black S et al. Comparative safety of two recombinant hepatitis b vaccines in children: data from the Vaccine Adverse Event Reporting System (VAERS) and Vaccine Safety Datalink (VSD). J Clin Epidemiol. 1998; in press.
28. Baraff LJ, Cody CL, Cherry JD: DTP-associated reactions: an analysis by injection site, manufacturer, prior reactions, and dose. Pediatrics 1984; 73:31-6.
29. Rastogi SC ed. International Workshop:Harmonization of Reporting of Adverse Events Following Vaccination. Rockville MD: FDA/CBER, 1993.
30. Wiholm BE, Olsoon S, Moore N, Wood S. Spontaneous reporting systems outside the U.S. In: Strom BL, ed. Pharmacoepidemiology. Sussex: John Wiley & Sons, 1994:139-55..
31. Centers for Disease Control. National Childhood Vaccine Injury Act: Requirements for Permanent Vaccination Records and for Reporting of Selected Events after Vaccination. MMWR 1988;37:197-200.
32. Stetler HC, Mullen JR, Brennan JP, Livengood JR, Orenstein WA, Hinman AR. Monitoring System for Adverse Events Following Immunization. Vaccine. 1987;5:169-174.
33. Braun MM, Ellenberg SS. Descriptive epidemiology of adverse events following immunization: reports to the Vaccine Adverse Event Reporting System (VAERS), 1991-1994. J Pediatr 1997; in press.
34. Fenichel GM, Lane DA, Livengood JR, Horwitz SJ, Menkes JH, Schwartz JF: Adverse events following immunization: assessing probability of causation. Pediatr Neurol 1989; 5:287-90.
35. Wassilak SGF, Sokhey J: Monitoring of adverse events following immunization in the Expanded Programme on Immunization. World Health Organization 1991; WHO/EPI/GEN/91.2:1-29.
36. Kramer MS, Lane DA. Causal propositions in clinical research and practice. J Clin Epidemiol 1992; 45:639-49.
37. Mariner WK: Compensation programs for vaccine-related injury abroad: a comparative analysis. Saint Louis University Law Journal 1987; 31:599-654.
38. Forsey T, Mawn JA, Yates PJ, Bently ML, Minor PD. Differentiation of vaccine and wild mumps viruses using the polymerase chain reaction and dideoxinucleotide. J Gen Virol 1990;71:987-90.
39. Henderson DA, Witte JJ, Morris L, Langmuir AD. Paralytic disease associated with oral polio vaccines. JAMA 1964;190:153-60.
40. Ray WA, Griffin MR. Confounding in studies of adverse reactions to
vaccines (letter). Am J Epidemiol 1994;139:229.
41. Davis R, Vadheim C,
Black S, et al. Immunization tracking systems: experience of the CDC Vaccine
Safety Datalink sites. HMO Practice 1997;11:13-7.
42. Black S.B., Shinefield H.R., and the Northern California Permenente Medical Care Program Department of Pediatrics Vaccine Study Group. b-CAPSA I Haemophilus influenzae, typeb capsular polysaccharide vaccine safety. Pediatrics 1987;79:321- 325.
43. Williams JC, Goldenthal KL, Burns DL, Lewis BP Jr, eds. Combined vaccines and simultaneous administration: current issues and perspective. New York: New York Academy of Science; 1995.
44. Hinman AR, Orenstein WA. Public health considerations. In: Plotkin SA, Mortimer EA, eds. Vaccines. Philadelphia: WB Saunders; 1994: 903-932.
45. Evans G. Vaccine liability and safety: a progress report. Pediatr Infect Dis J 1996:15:477-8.
46. Walker AM, Jick H, Perera DR, et al. Neurologic events following diphtheria-tetanus-pertussis immunization. Pediatrics. 1988;81:345-349.
47. Griffin MR, Ray WA, Mortimer EA, et al. Risk of seizures and encephalopathy after immunization with the diphtheria-tetanus-pertussis vaccine. JAMA. 1990;263:1641-1645.
48. Fine PEM. Methodological issues in the evaluation and monitoring of vaccine safety. Ann NY Acad Sci 1995; 754:300-8.
49. Watson JC, Peter G. General Immunization Practices. In: Plotkin SA, Orienstein WA (eds). Vaccines 3rd edition. WB Saunderes, Philladelphia, 1998. (In Press).
50. American Academy of Pediatrics. Active immunization. In: Peter G, ed 1997 Redbook:Report of the Committee on Infectious Diseases. 24th ed. Elk Grove Village, IL:American Academy of Pediatrics;1997:4-36.
51. U.S. Department of Health and Human Services, Public Health Service, CDC. Vaccine management recommendations for handling and storage of selected biologicals. March 1991.
52. U.S. Department of Health and Human Services, Public Health service, CDC. Guidelines for vaccine packing and shipping. January 1997.
53. Weniger BG, Chen RT, Jacobsen SH, Sewell EC, Dueson R, Livengood JR, et al. Addressing the challenges to immunization practice with an economic algorithm for vaccine selection. Vaccine, 1998, in press.
54. Zaffran M, Lloyd J, Clements J, Stilwell. A drive to safer injections. Geneva: WHO/GPV/SAGE.97/WP.05, 1997.
55. Orenstein WA. DTP vaccine litigation, 1988. Am J Dis Child 1990;144:517.
56. Institute of Medicine: Liability for the production and sale of vaccine. In: Vaccine supply and innovation. Wash D.C.: National Academy Press, 1985; 85-122.
57. Offit PM, Bell LM. What every parent should know about vaccines. Simon &Schuster Macmillan company. New York, NY 1998:1.
58. Freed GL, Katz SL, Clark SJ. Safety of vaccinations: miss American, the media, and public health. JAMA. 1996;276:1869-1872, 1917-1918.
59. Institute of Medicine: Risk Communication and Vaccination, Workshop summary. Wash D.C.: National Academy Press, 1997.
60. National Research Council. Improving risk communication. Washington DC: National Academy Press, 1989.
61. Fischhoff B, Bostrom A, Jacobs-Quadrel M. Risk perceptions and
communcation. Annual Review of Public Health 1993;14:182-203
62. Hibbs
BF, Wolfe S, Chen RT. Internet Web page perceptions of vaccine
pharmacoepidemiology research: an analysis of vaccine safety concerns. Abstract
129. Abstracts of the 13th International Conference on
Pharacoepidemiology. Walt Disney World, Florida: August 24-27, 1997.
Pharmacoepidemiology and Drug Safety. 1997; 6 (suppl 2): S60.
63. Meszaros JR, Asch DA, Baron J, Hershey JC, Kunreuther H, Schwartz-Buzaglo J. Cognitive processes and the decisions of some parents to forego pertussis vaccination for their children, Journal of Clinical Epidemiology 1996;49:697-703.
64. Hance BJ, Chess C, Sandman P. Industry risk communication manual. Chelsea, MI. Lewis Publishers 1990.
65. The National Childhood Vaccine Injury Act of 1986, at Section 2125 of the Public Health Service Act as codified at 42 U.S.C. § 300aa-(Supp.1987).
66. Tversky A, Kahneman D. Availability:A Heuristic for judging frequencey and probability. Cognitive Psychology 1973;5:207-232.
67. Baron J. The effect of normative beliefs on anticipated emotions. Journal of Personality and Social Psychology 1992;63:320-330.
68. Bostrom A. Vaccine Risk Communication:Lessons from Risk Perception, Decision making and Environmental Risk Communication Research. 8 Risk: Health, Safety&Environment 173: Spring 1997:173-200.
69. Binkin NJ et al. Epidemiology of Pertussis in a developed country with
low vaccination coverate:the Italian Experience. 1992. Pediatr. Infect. Dis. J.
11:653.